
Unsure When You Can Return to Play?
Last summer, researchers from the American Orthopedic Society of Sports Medicine (AOSSM) held their their annual meeting. The topic? ACL injuries in youth sports. The major discussion point was the standards on return-to-play protocols for these athletes. The current standard of assessing readiness following an ACL repair does not seem to be adequate. In their discussion, they review a study performed by a number of elite-level researchers. They are looking at the incidence of 2nd ACL injuries in 13-25 years old.
How Often Does This Happen?
In this age-range, the re-injury rates range from 25-33%. Most of which happen in the first 12 months following a repair. This number is quite concerning! According to this research, 117 out of 159 athletes assessed did not meet traditional return-to-play guidelines. Without being properly assessed for readiness, 117 athletes were allowed to return to play. This is a huge deal and is likely the reason the re-injury rate is so high in this population, unfortunately.
We seem to run into the same problem every time!
There is no general consensus or follow-through when it comes to monitoring the rehab process. This is especially following surgery, nor does there seem to be thorough testing done with this population. I often hear that an athlete’s doctor or PT used more of a time-based approach to releasing the athlete. They were cleared to play once they reached 6 or 9 months.
This is an issue as every athlete is different in their healing process as well as recovery process. Some athletes don’t even start introducing plyometrics or skill-based work until 5-6 months (as they’re reluctant or fearful). How could we allow them to start playing a sport that involves jumping and cutting? Then we have the athletes who are more progressive with their rehab. How do we know that they’re loading the injured side the same as the non-injured side? How do we know that athlete has adequate strength, neuromuscular control and coordination, and force output? This is where monitoring and testing come into play, and where the lab at Greenwich Sports Medicine stands out.
Image provided by Matt Jordan, PhD of Jordan Strength
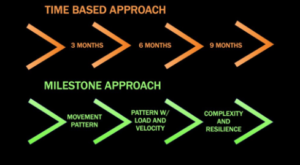
Here at GSM,
we’re utilizing our state-of-the-art Biomechanics Lab. Not only to test our athletes before they play again, but to monitor them throughout the process too. We use a milestone-based approach as outlined in the diagram (left). We observe their movement patterns, test their loading parameters and velocities. Then we record and study complex tasks once progressed to that level. The rehabilitation process isn’t always provided by us. However, our ability to monitor these progressions is the major key. This helps us in partnering with other facilities that don’t have the available technology that we have.
Our return-to-play testing is multifactorial in nature. Looking at everything from the forces created with jumping and landing, to balance and stability. We are also looking at running mechanics and other ‘sport-specific’ activities. All measured and scored objectively. This sets our testing apart from what it appears others are doing. We’re able to quantify every move an athlete makes, rather then guess and blindly make a decision. This is of extreme importance for these athletes. Not having data to support our decisions ends up leading to these high rates of re-injury, and no one wants that.
Interested in preventing re-injury? Give our office a call today!
Dr. Alex Svac